
A 1-month-old boy is evaluated for poor feeding. When nursing, the patient becomes diaphoretic, and, for the past week, he has fed for only 5 minutes at a time before falling asleep. Today, his weight is 30 g (1 oz) below birth weight. Vital signs are normal. Examination shows a thin infant who is sleeping but easily arousable. Cardiac examination demonstrates tachycardia with a 1/6 holosystolic murmur over the left lower sternal border and diastolic rumble over the cardiac apex. S2 is prominent. The patient is tachypneic, but lung fields are clear to auscultation. There is no clubbing, cyanosis, or peripheral edema. Which of the following is the most likely cause of this patient's symptoms?
| A. Atrial septal defect | ||
| B. Mitral stenosis | ||
| C. Tetralogy of Fallot | ||
| D. Transposition of the great vessels | ||
| E. Ventricular septal defect |
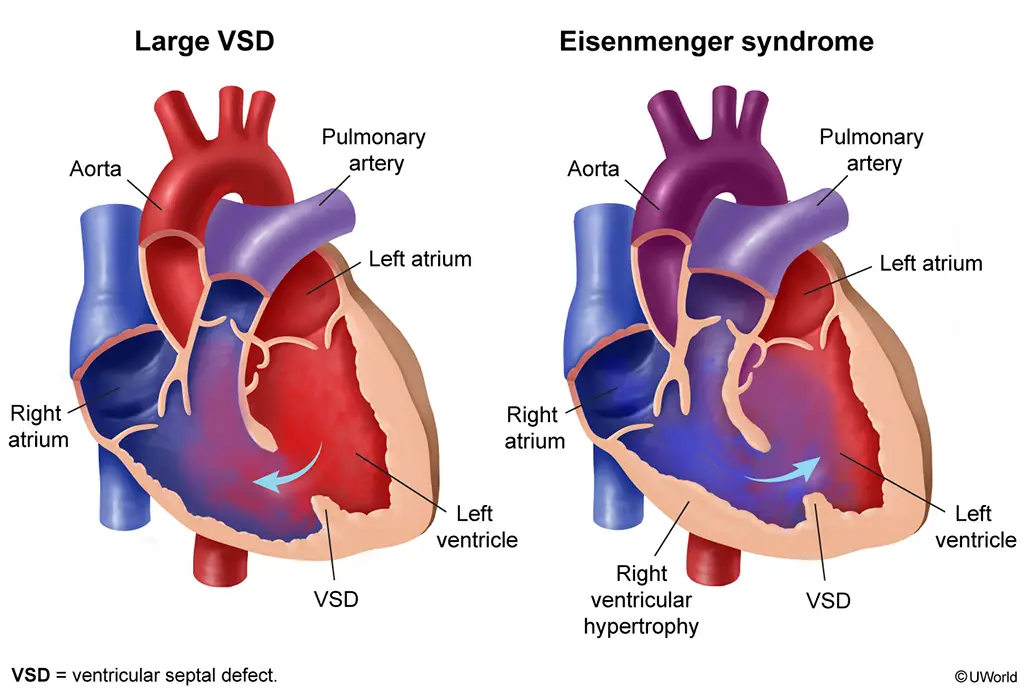
This patient's examination is most consistent with a large ventricular septal defect (VSD), a common congenital heart malformation. VSDs range from small and asymptomatic to large with significant left-to-right shunting. Features include the following:
- The characteristic murmur is holosystolic at the left lower sternal border. Small or moderate VSDs produce louder holosystolic murmurs due to turbulence. In contrast, large VSDs are quieter due to lower resistance (and less turbulence) through a larger orifice.
- An apical diastolic rumble may also be heard from increased flow across the mitral valve (as a result of increased left-to-right shunting across the VSD).
- As right ventricular pressure increases (due to increased flow), the S2 becomes more prominent (due to increased pressure closing the pulmonary valve).
Significant left-to-right shunting results in pulmonary overcirculation and pulmonary hypertension, growth failure, diaphoresis, easy fatigability, and congestive heart failure. Unrepaired, large VSDs result in permanent pulmonary hypertension, which leads to shunt reversal (ie, right to left rather than left to right) with cyanosis (Eisenmenger syndrome). Echocardiography confirms the defect's size and location. Treatment of large VSDs generally combines medications (eg, diuretics) and defect closure.
(Choice A) A large atrial septal defect can cause tachypnea. However, it would lead to a widened and fixed S2, which is not present in this patient.
(Choice B) Mitral stenosis also causes an apical diastolic rumble but not a holosystolic murmur at the left lower sternal border.
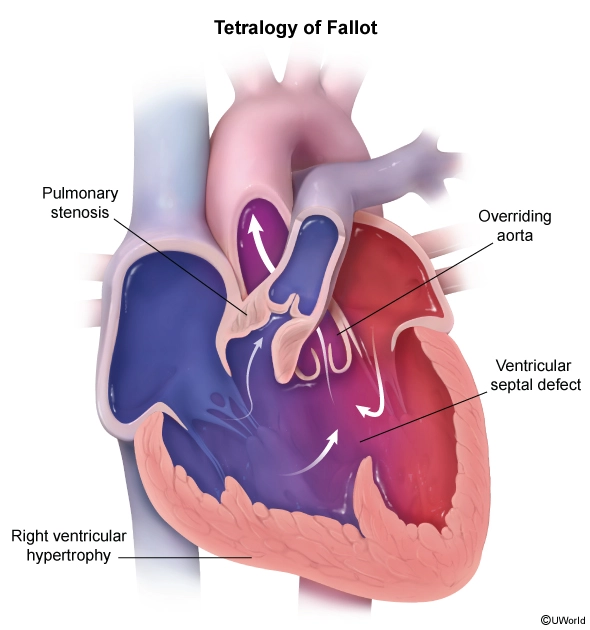
(Choice C) Tetralogy of Fallot consists of a VSD, right ventricular outflow tract obstruction (eg, pulmonic stenosis), overriding aorta, and right ventricular hypertrophy. The pulmonary stenosis component causes a harsh systolic ejection murmur at the left upper sternal border.
(Choice D) Transposition of the great vessels is characterized by the aorta arising from the right ventricle and the pulmonary artery arising from the left ventricle. It would cause cyanosis, which is not seen in this patient.
Educational objective:
Large ventricular septal defects cause growth failure, pulmonary hypertension, and heart failure. They classically produce a holosystolic murmur that is loudest at the left lower sternal border and an apical diastolic rumble due to increased blood flow across the mitral valve.
A 68-year-old man comes in due to 2 months of bulky, foul-smelling diarrhea. The patient reports that his stools appear oily in character and are difficult to flush. He has also had intermittent, epigastric abdominal pain for the past 6 months that has not improved with a proton pump inhibitor trial. The patient has had no melena, nausea, or vomiting, but he has lost 7 kg (15.4 lb) over the last 6 weeks. He drinks 5 or 6 beers daily and has a 20-pack-year history. On physical examination, the epigastrium is mildly tender to palpation but is without distension, rebound tenderness, or guarding. Which of the following is most likely to establish the diagnosis in this patient?
| A. Anti–tissue transglutaminase antibodies | ||
| B. CT scan of the abdomen | ||
| C. Lactose breath hydrogen test | ||
| D. Serum amylase | ||
| E. Upper gastrointestinal endoscopy |
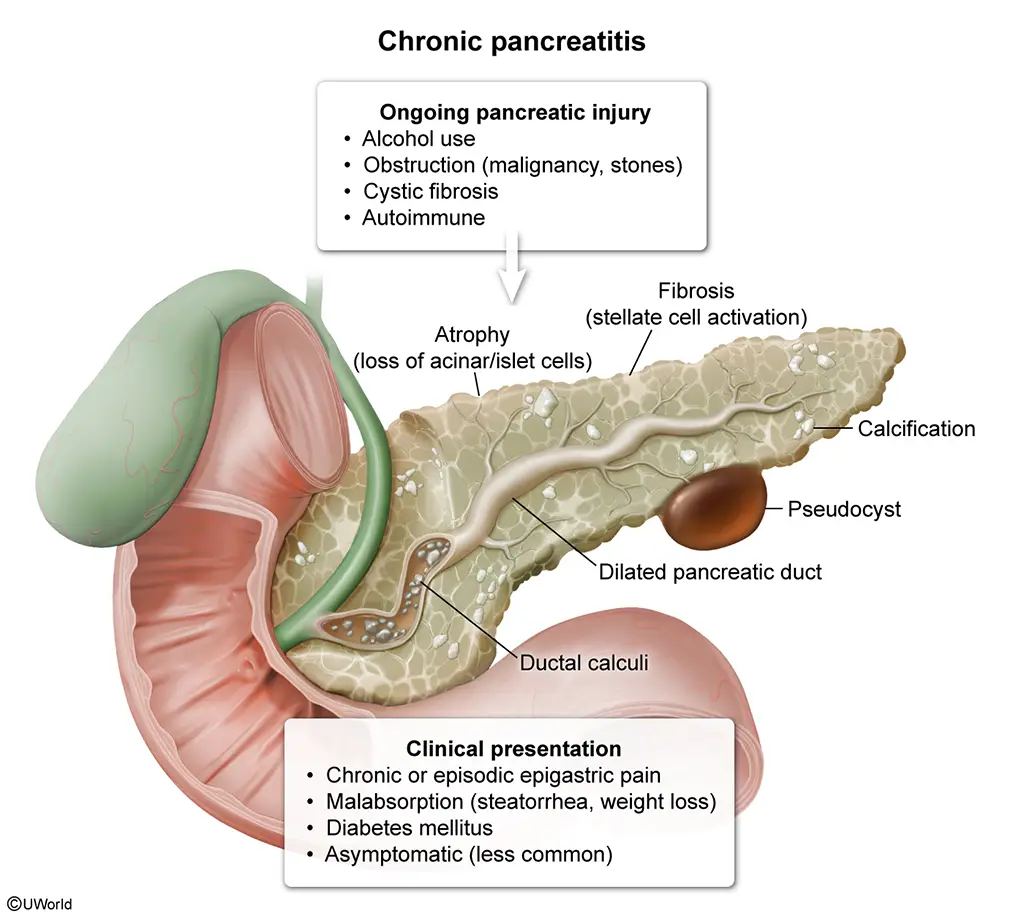
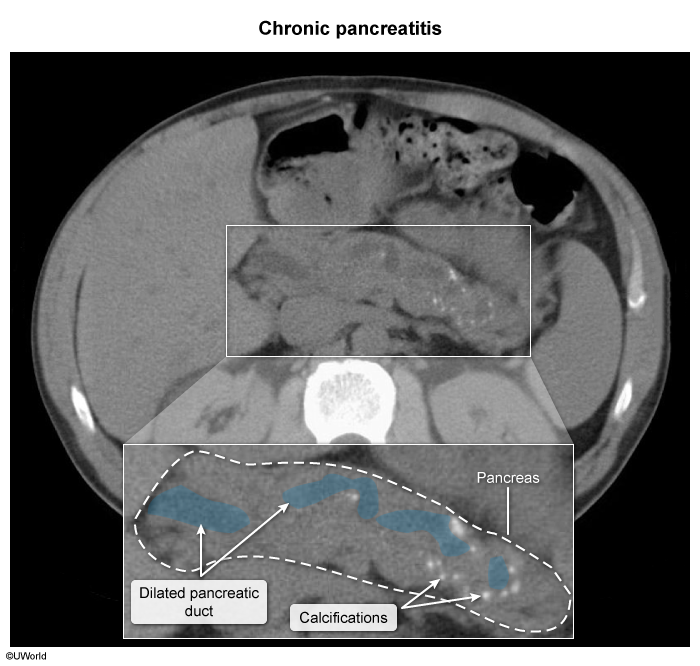
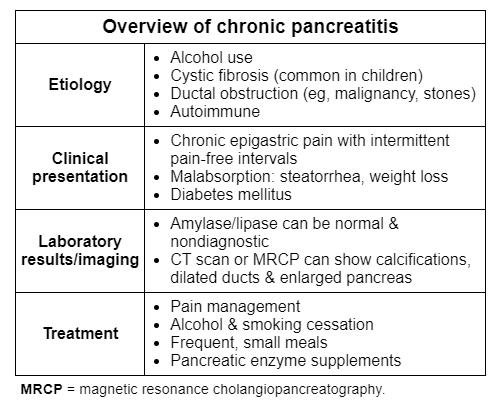
This patient's weight loss, abdominal pain, and steatorrhea (bulky, oily, foul-smelling stools often difficult to flush) are suggestive of chronic pancreatitis, defined as progressive pancreatic inflammation with permanent structural damage and resultant endocrine and exocrine dysfunction. Risk factors for chronic pancreatitis include alcohol use (most common), genetics (eg, cystic fibrosis), pancreatic ductal obstruction (eg, malignancy, stones), and autoimmune disease. Patients usually have episodic or daily abdominal pain and findings of pancreatic insufficiency (eg, malabsorption, diabetes mellitus).
Pancreatic fibrosis leads to decreased enzyme levels within the pancreas; as a result, serum amylase and lipase levels are usually normal and nondiagnostic (Choice D). Plain abdominal radiographs reveal calcifications within the pancreatic duct in only 30% of patients. Abdominal CT scan and MR cholangiopancreatography are the preferred diagnostic modalities because they are more sensitive and can readily show calcifications, dilated ducts, pancreatic atrophy, or fluid collections (pseudocyst). Treatment involves pancreatic enzyme replacement, which includes lipase to aid in fat digestion and improve steatorrhea.
(Choice A) Anti–tissue transglutaminase antibodies are present in celiac disease, which is due to gluten enteropathy and may be associated with an increased risk for chronic pancreatitis. Celiac disease can be asymptomatic or present with steatorrhea, weight loss, iron deficiency anemia, nutritional deficiencies (eg, vitamins D and B12), and metabolic bone disease. However, it usually does not cause significant abdominal pain, as seen in this patient.
(Choice C) Lactose breath hydrogen testing aids in the diagnosis of lactose intolerance, which typically presents with abdominal pain, bloating, flatulence, and diarrhea (eg, bulky, frothy, watery stools) following lactose ingestion (eg, milk). Weight loss is atypical, and this patient's alcohol intake makes chronic pancreatitis more likely.
(Choice E) Upper gastrointestinal endoscopy can effectively diagnose gastric, duodenal, and esophageal pathology (eg, malignancy, ulcers, inflammation). However, this patient has no evidence of dysphagia, vomiting, or melena to suggest an upper gastrointestinal disorder.
Educational objective:
Chronic pancreatitis usually presents with episodic or daily abdominal pain and findings of pancreatic insufficiency (eg, diabetes mellitus, steatorrhea, weight loss). Chronic alcohol consumption is the most associated risk factor. Diagnosis is typically confirmed with abdominal CT scan or MR cholangiopancreatography showing calcifications, dilated ducts, and pancreatic atrophy.
- Pancreatitis
A 54-year-old man comes to the office due to daytime sleepiness and lack of energy. The symptoms began 6 months ago and have progressively worsened so that he feels "completely drained" by the end of the day. The patient's wife mentions that he snores loudly. He has not had a medical evaluation in over 10 years. BMI is 34 kg/m2. Physical examination shows a narrow oropharynx and a large neck circumference. This patient is at increased risk of developing which of the following?
| A.Bronchiectasis | ||
| B. Hypertrophic cardiomyopathy | ||
| C. Laryngeal carcinoma | ||
| D. Narcolepsy | ||
| E. Pulmonary hypertension |
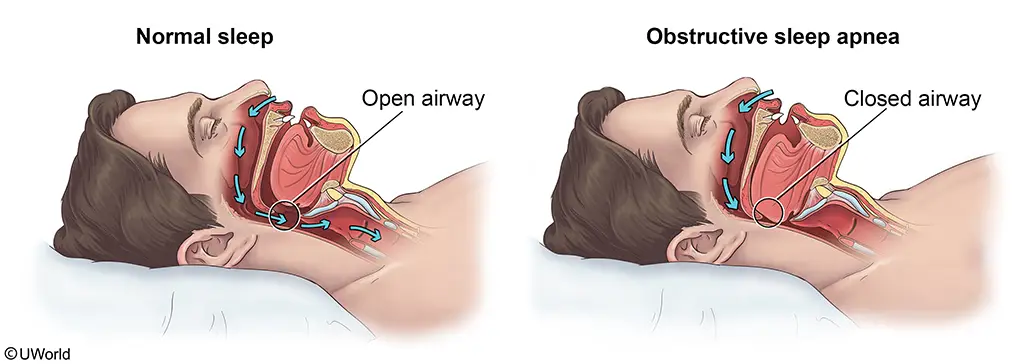
This patient, an obese man with loud snoring, daytime sleepiness, and suggestive examination findings (eg, thick neck, narrow airway) most likely has obstructive sleep apnea (OSA). OSA is characterized by recurrent obstruction of the upper airway during sleep; each nocturnal episode of reduced ventilation causes transient hypercapnia and hypoxemia. These blood gas derangements result in reflexive systemic and pulmonary vasoconstriction, endothelial dysfunction, abnormal venous return and cardiac output, and sympathetic cardiac stimulation.
Prolonged, untreated OSA can cause pulmonary hypertension and right heart failure. Most patients with OSA will develop systemic hypertension due to chronic sympathetic stimulation and elevated plasma norepinephrine levels. Patients also lose the normal diurnal variation in blood pressure. Other cardiovascular complications of OSA include atrial fibrillation and other arrhythmias, coronary artery disease, and increased risk of sudden cardiac death.
(Choice A) Acquired bronchiectasis may be seen in patients with recurrent infection, impaired drainage (eg, cystic fibrosis), or airway obstruction (eg, foreign body aspiration.
(Choice B) Systemic hypertension, as seen in OSA, can lead to mild-to-moderate left ventricular hypertrophy and impaired systolic and diastolic function. In contrast, hypertrophic cardiomyopathy is an autosomal dominant disease of the cardiac sarcomere characterized by severe myocardial hypertrophy. It is not associated with hypertension or OSA.
(Choice C) Laryngeal carcinoma is associated with cigarette smoking and heavy alcohol use.
(Choice D) Like OSA, narcolepsy can also cause daytime drowsiness. However, narcolepsy is also associated with cataplexy (sudden loss of muscle tone), sleep attacks, sleep paralysis, and hypnagogic hallucinations. OSA is not a risk factor for narcolepsy.
Educational objective:
Obstructive sleep apnea presents in obese individuals with excessive daytime sleepiness and signs of nocturnal upper airway obstruction (eg, snoring, gasping). The condition is associated with systemic hypertension. Prolonged, untreated obstructive sleep apnea can also cause pulmonary hypertension and right heart failure.
- Sleep disorders
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}