Cardiovascular System
The cardiovascular system is 13% of PANCE and 12% of PANRE. Cardiovascular is the largest content category tested on each exam. Test your exam readiness by trying a challenging sample question.
A 68-year-old man presents for myalgia and fatigue. The patient has been taking high-intensity statin therapy since he had an acute myocardial infarction several weeks ago. Other medical conditions include hypertension and type 2 diabetes mellitus. On examination, there is mild generalized muscle tenderness. Serum creatine kinase level is 456 U/L. Vitamin D and TSH levels are within normal range. Statin therapy is discontinued, and he is prescribed a medication that inhibits cholesterol absorption at the brush border of the small intestine. Which of the following drugs was most likely started in this patient?
| A. Colesevelam | ||
| B. Ezetimibe | ||
| C. Fenofibrate | ||
| D. Nicotinic acid | ||
| E. PCSK9 inhibitor |
Explanation:
Statin-associated muscle symptoms, rare adverse effects of statin therapy, typically begin within weeks to months after the initiation of statins, as in this patient. The clinical presentation encompasses myalgia, symmetric muscle weakness (often reported as fatigue), and rhabdomyolysis with an accompanied elevation of creatine kinase. In addition, serum vitamin D and TSH levels should be checked because low vitamin D and hypothyroidism increase susceptibility to statin-associated myopathy.
Treatment is to stop the offending statin. In high-risk patients, such as those with coronary artery disease, another cholesterol-lowering agent with a more favorable adverse effect profile can be used to help reduce the risk for reinfarction.
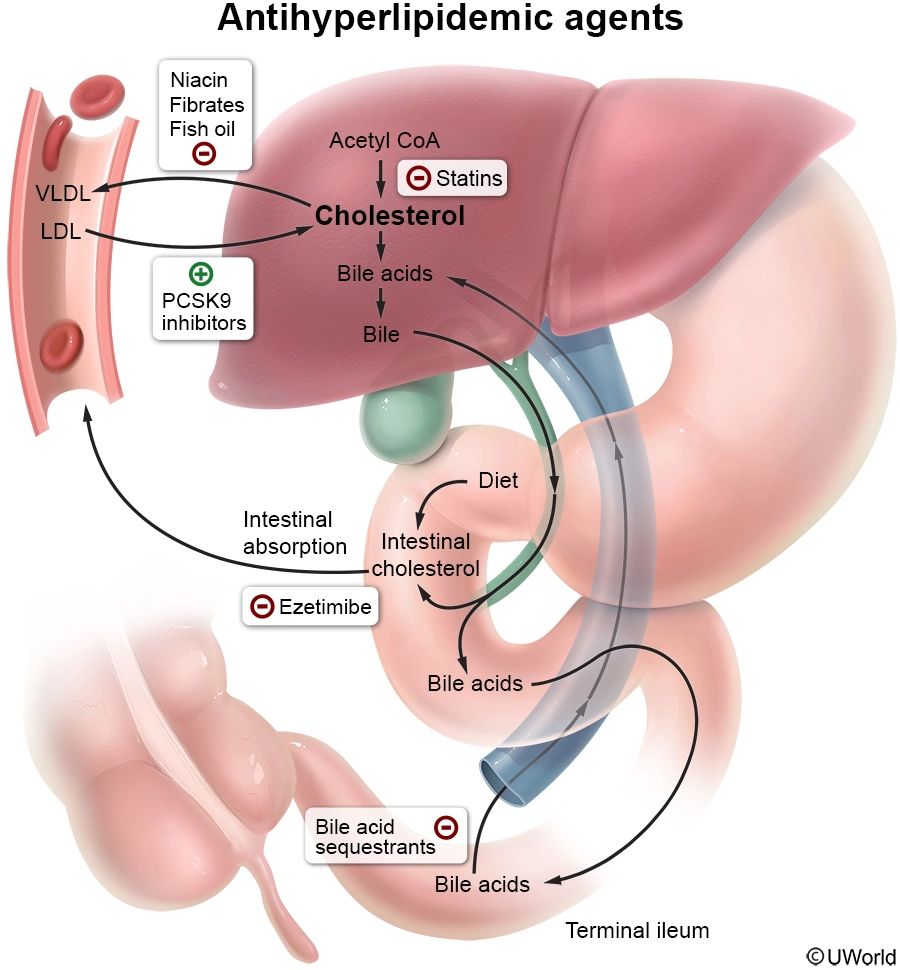
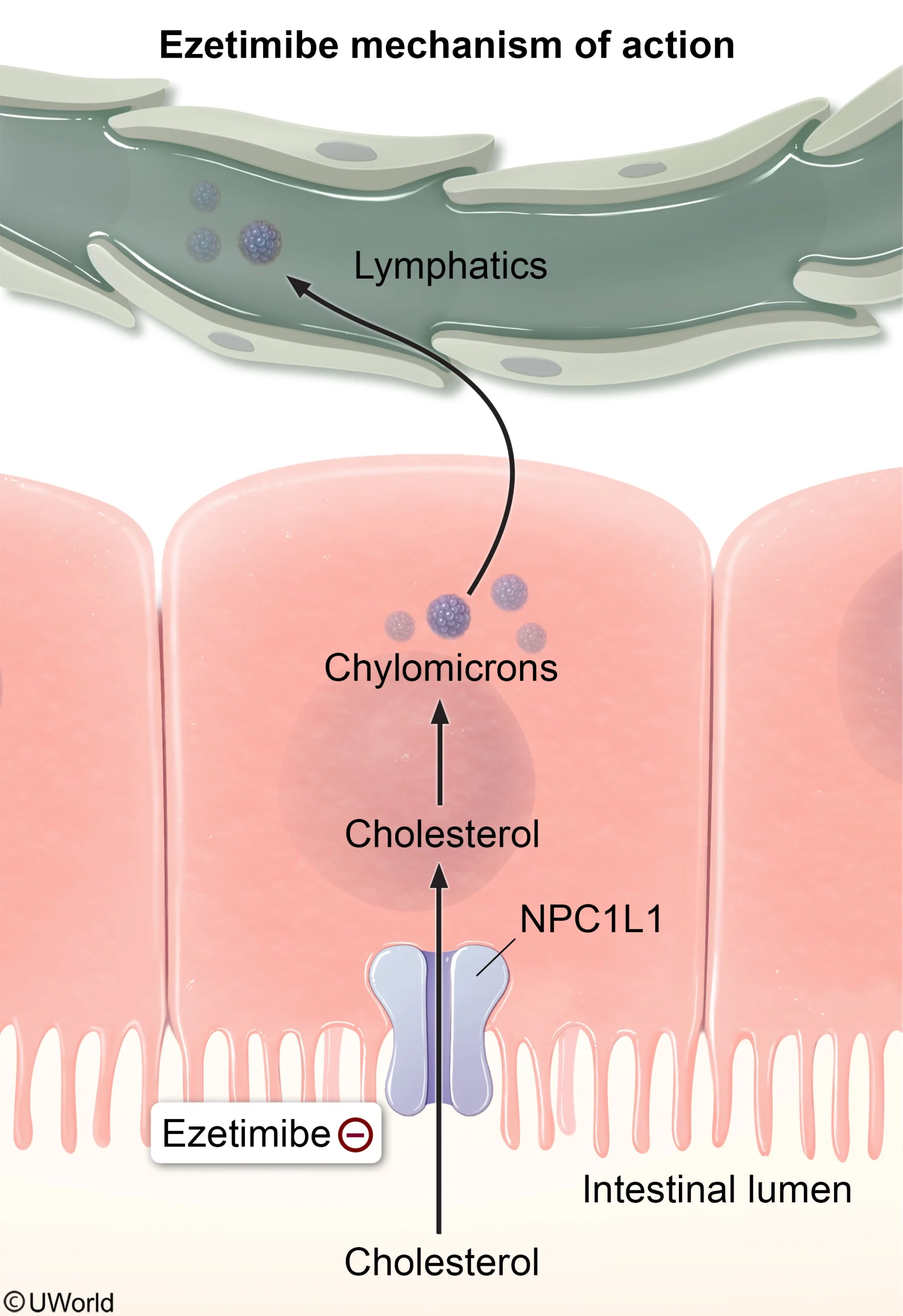
Ezetimibe decreases the intestinal absorption of cholesterol by inhibiting the transport of dietary cholesterol from the gastrointestinal lumen into intestinal enterocytes. As a result, the total amount of dietary cholesterol reaching the liver decreases, lowering intrahepatocyte cholesterol levels. To compensate, the liver increases LDL receptor expression, which draws cholesterol out of the circulation.
{kind=link}
(Choice A) Bile acid sequestrants (eg, colesevelam) bind bile salts in the intestine, decreasing their reabsorption. Subsequent depletion of the bile acid pool favors the conversion of cholesterol into bile acids.
(Choice C) Fibrates (eg, fenofibrate) reduce hepatic triglyceride production and increase lipoprotein lipase activity, which, in turn, increases the breakdown of triglyceride-rich lipoproteins. A favorable adverse effect of fibrates is an increase in HDL synthesis.
(Choice D) Nicotinic acid inhibits hepatic triglyceride synthesis, which, in turn, reduces the liver's availability to synthesize VLDL particles that are subsequently metabolized into LDL in the circulation.
(Choice E) Proprotein convertase subtilisin/kexin 9 (PCSK9) increases the degradation of hepatic LDL receptors. Alirocumab is a monoclonal antibody against PCSK9 that blocks this effect, resulting in increased availability of LDL receptors on hepatocyte membranes and, subsequently, increased clearance of LDL from the blood.
Educational objective:
Statin-associated muscle symptoms can present with myalgia, symmetric muscle weakness, and rhabdomyolysis. When these occur, the statin should be stopped, and patients may be switched to a nonstatin medication such as ezetimibe. Ezetimibe works by decreasing the intestinal absorption of cholesterol.
Pulmonary System
The pulmonary system makes up 10% of PANCE and PANRE. See if you can answer this free pulmonary system exam question.
A newborn boy is admitted due to respiratory distress. He was born to a 34-year-old primigravida whose pregnancy was complicated by type 1 diabetes mellitus. The boy was born via cesarean delivery after a prolonged labor. Weight is 4700 g (10 lb 6 oz). Physical examination immediately after delivery shows tachypnea, nasal flaring, and intercostal retractions. Pulse oximetry is 78% on room air. The infant is intubated and mechanical ventilation is started. High pressures are required to achieve normal tidal volume and keep the alveoli inflated. This infant's condition is caused by dysfunction of which of the following?
| A. Fibroblasts | ||
| B. Macrophages | ||
| C. Type 1 pneumocytes | ||
| D. Type 2 pneumocytes | ||
| E. Vascular smooth muscle |
Explanation:
This patient has neonatal respiratory distress syndrome (RDS), a condition caused by insufficient surfactant. Although prematurity is the greatest risk factor for RDS, poorly controlled diabetes mellitus also increases the risk due to maternal hyperglycemia, which leads to fetal hyperglycemia (macrosomia) and hyperinsulinism; high insulin levels antagonize the effects of cortisol, causing delayed lung maturation and reduced surfactant production.
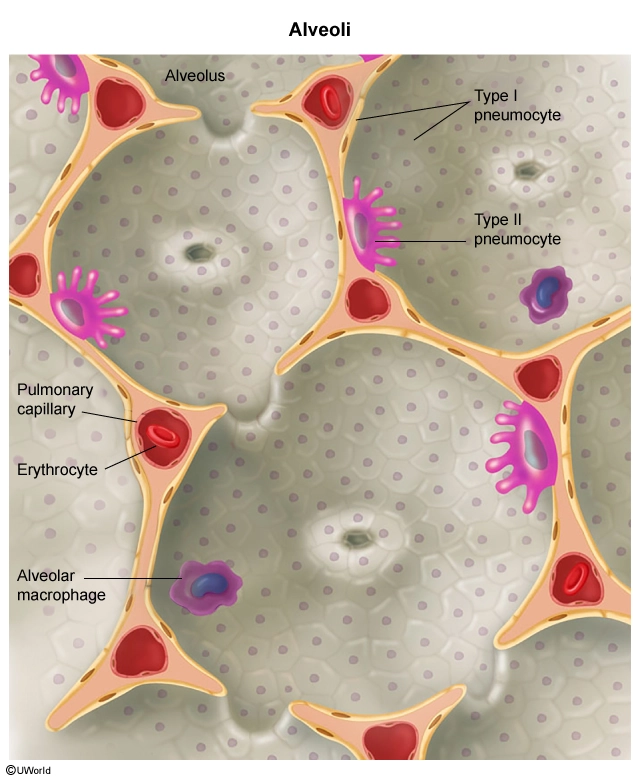
Surfactant is a lipoprotein complex produced by type 2 pneumocytes that reduces alveolar surface tension; inadequate surfactant leads to poor lung compliance and diffuse alveolar collapse. Patients with RDS develop respiratory distress soon after birth, often requiring high airway pressures to prevent atelectasis. Subsequent injury to cells within the alveolar epithelium results in alveolar deposition of fibrin, protein, and cellular debris (ie, hyaline membranes).
Treatment includes respiratory support and exogenous surfactant. Antepartum corticosteroids are administered to women at risk of preterm delivery to mature fetal type 2 pneumocytes and decrease the risk for RDS. Infants who survive the initial stages of RDS recover in 3-7 days, as their type 2 pneumocytes begin to secrete normal amounts of surfactant.
(Choice A) Fibroblasts produce inappropriate connective tissue in many restrictive lung diseases (eg, idiopathic pulmonary fibrosis, chemotherapy- or radiation-induced lung disease). RDS is a restrictive lung disease (eg, decreased volumes, normal exhalation) but is not mediated by fibroblasts.
(Choice B) Macrophages form pulmonary granulomas in sarcoidosis and Mycobacterium tuberculosis infections. They are not involved in the pathogenesis of RDS.
(Choice C) Type 1 pneumocytes form the majority of the alveolar membrane and are separated from the endothelial cells of the pulmonary capillaries by a thin basement membrane. Type 1 pneumocytes are damaged (not the cause of) in neonatal RDS.
(Choice E) Failure of the pulmonary smooth muscle cells to relax after delivery causes persistent pulmonary hypertension in the newborn. This most commonly follows meconium aspiration syndrome. It does not cause RDS.
Educational objective:
Respiratory distress syndrome occurs when type 2 pneumocytes produce insufficient amounts of surfactant, causing increased alveolar surface tension and decreased lung compliance. Surfactant deficiency is common in premature infants but can also occur in infants of diabetic mothers.
Gastrointestinal System/Nutrition
The gastrointestinal system is 9% of PANCE and 10% of PANRE. Check your esophageal disorders knowledge with this exam-like practice question.
A 54-year-old man presents with difficulty swallowing solids but not liquids for the past 3 months. The patient frequently has a sensation of food "sticking" within the chest, which is worse with solid foods. He has no choking, coughing, or vomiting while eating. Medical history is significant for gastroesophageal reflux disease for the past 6 years managed with antireflux therapy. An endoscopy 6 months ago revealed Barrett esophagus without dysplasia. BMI is 38 kg/m2. Repeated imaging reveals an area of symmetric, concentric narrowing affecting the distal esophagus. Which of the following is the most likely diagnosis?
| A. Achalasia | ||
| B. Esophageal stricture | ||
| C. Esophageal web | ||
| D. Hiatal hernia | ||
| E. Vascular ring |
Explanation:
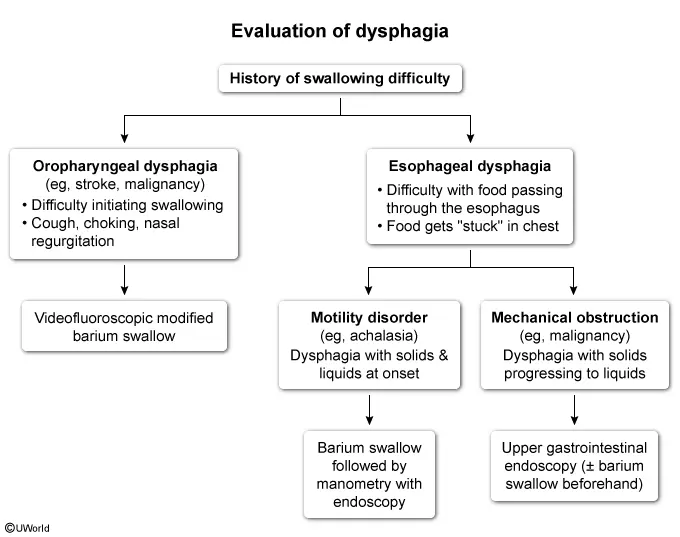
This patient with chronic gastroesophageal reflux disease (GERD) has esophageal dysphagia, which is characterized by normal initiation of a swallow (eg, no choking, coughing) followed by a sensation that food "sticks" within the chest. Difficulty swallowing solids but not liquids is characteristic of mechanical obstruction.
{kind=link}
Common causes of mechanical obstruction in patients with GERD include the following:
-
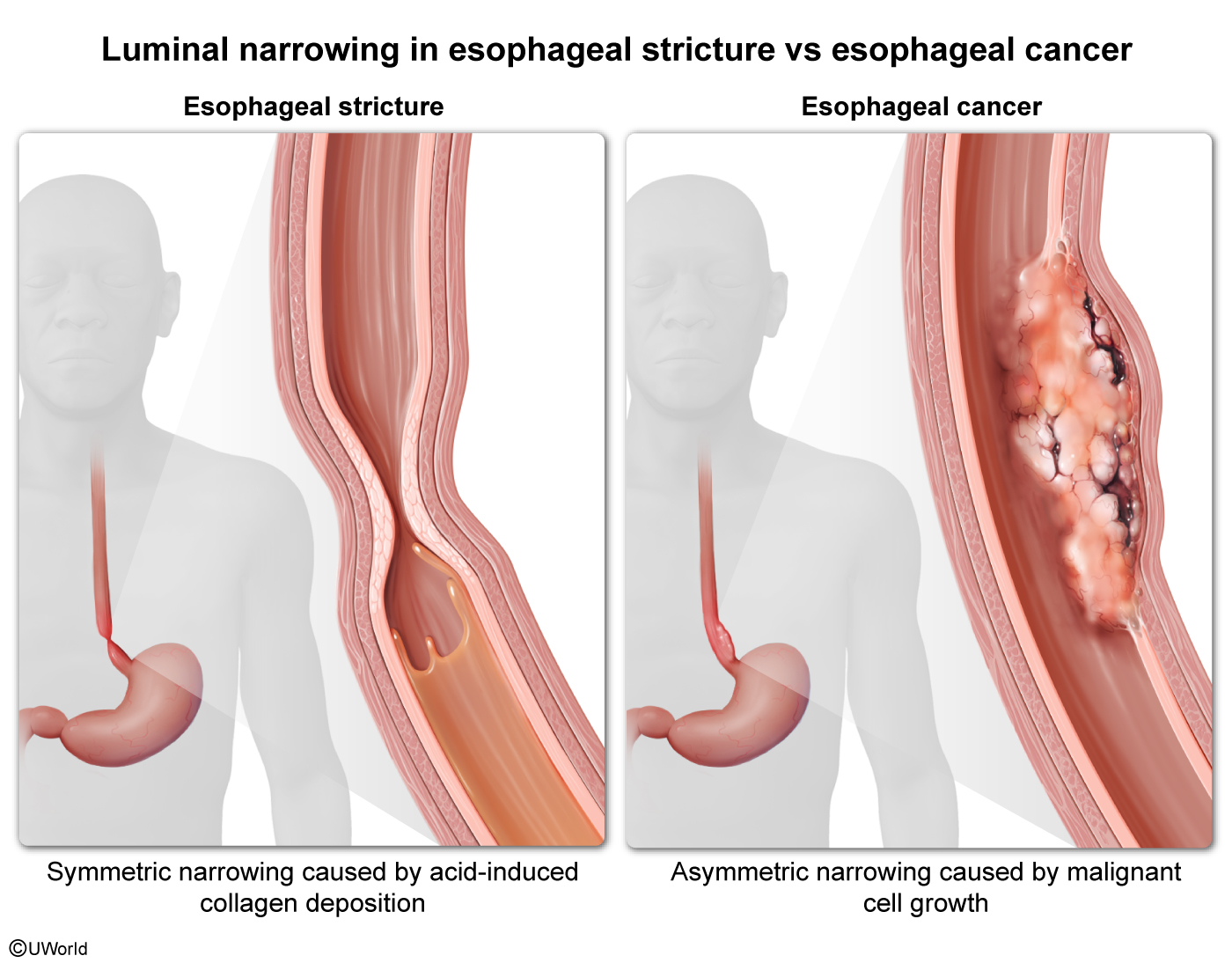
Esophageal stricture, which is caused by reparative collagen deposition in response to esophageal mucosal damage caused by acidic gastric contents. Most strictures are not malignant and typically cause slowly progressive dysphagia to solid foods without anorexia or weight loss. On endoscopy, they are seen as concentric narrowings in the distal esophagus and are generally symmetric.
-
Esophageal adenocarcinoma, which can occur in a small percentage of patients with Barrett esophagus (BE) (intestinal metaplasia in the distal esophagus). On endoscopy, they are typically seen as an asymmetric and irregular narrowing of the distal esophagus.
This patient likely has an esophageal stricture, which can be treated with endoscopic dilation. Although he was diagnosed with BE, there is no dysplasia, and adenocarcinoma is unlikely due to the slow rate of malignant transformation of BE (<1% per year; this patient's condition was diagnosed only 6 months ago) and inconsistent endoscopic findings of concentric, symmetric narrowing.
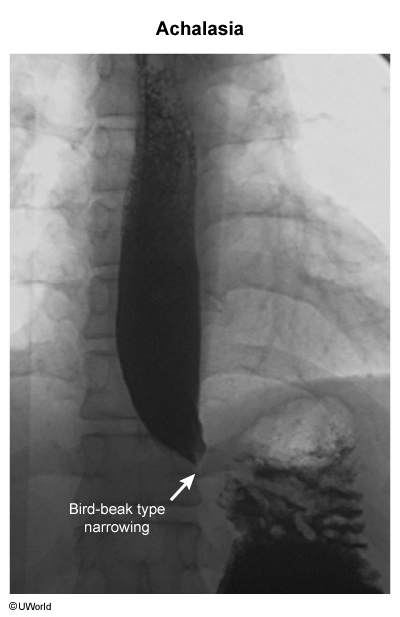
(Choice A) Achalasia is a motility disorder. Unlike a condition that causes mechanical obstruction (eg, esophageal stricture), achalasia presents with dysphagia to solids and liquids at onset, a feature not seen in this patient. Barium swallow typically shows aperistalsis, dilation of the esophagus proximal to the lower esophageal sphincter, and narrowing in a bird-beak pattern at the sphincter.
{kind=link}
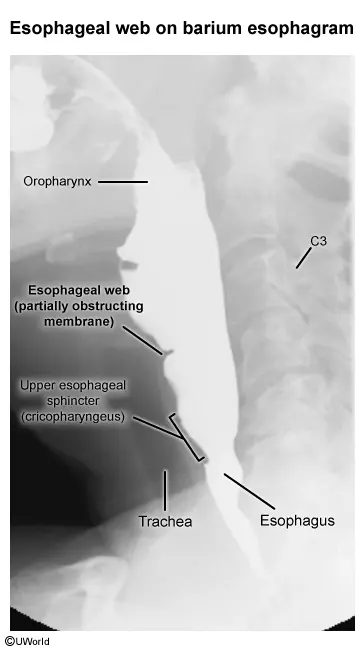
(Choice C) Esophageal webs are thin membranes of esophageal tissue that can obstruct the esophageal lumen. They often occur in a triad with iron deficiency anemia and dysphagia to solids foods (Plummer-Vinson syndrome). Esophageal webs are most commonly located in the upper, not lower, esophagus and cause only mild focal narrowing.
{kind=link}
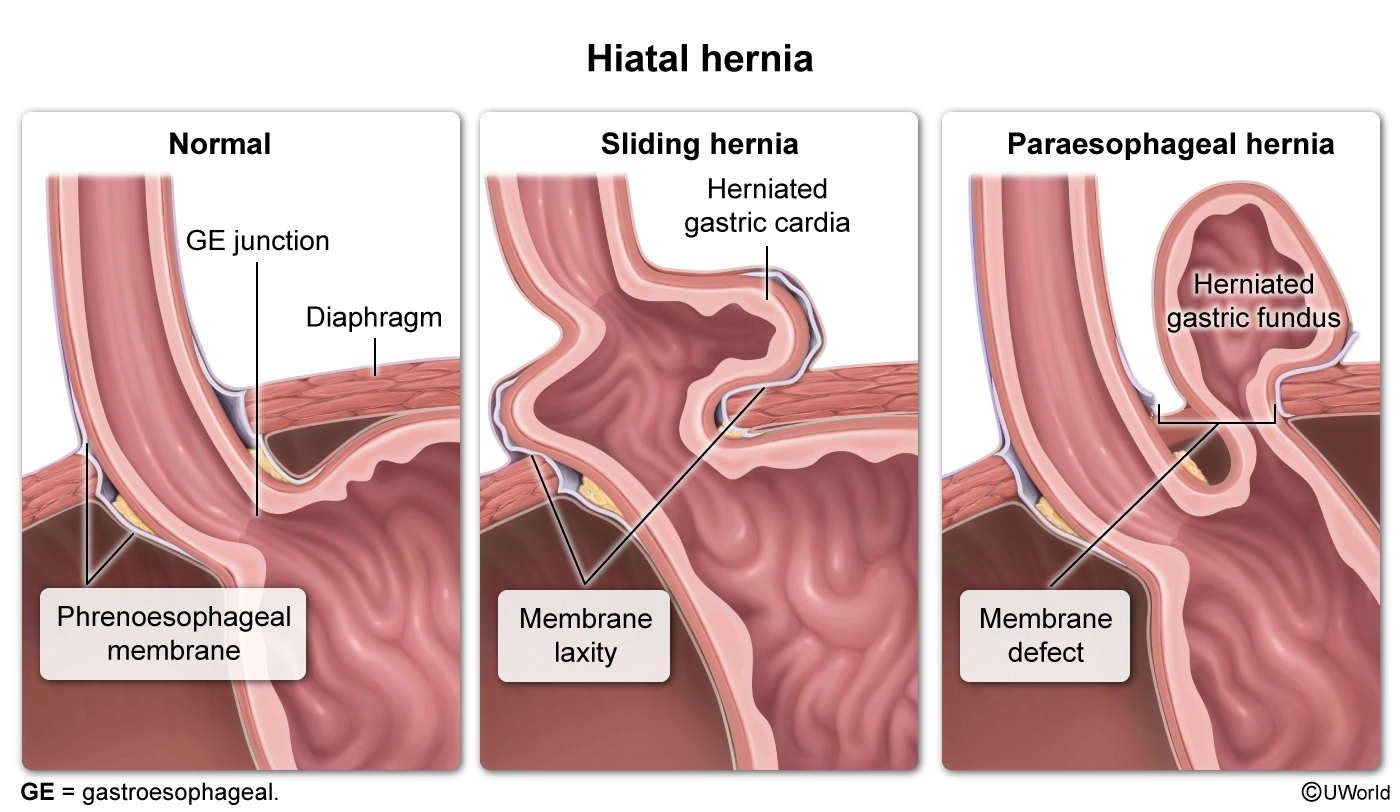
(Choice D) A hiatal hernia is a protrusion of the stomach above the diaphragm and can present with GERD (and related complications) due to an incompetent lower esophageal sphincter caused by anatomic distortion. However, barium swallow would reveal gastric folds protruding above the diaphragm.
{kind=link}
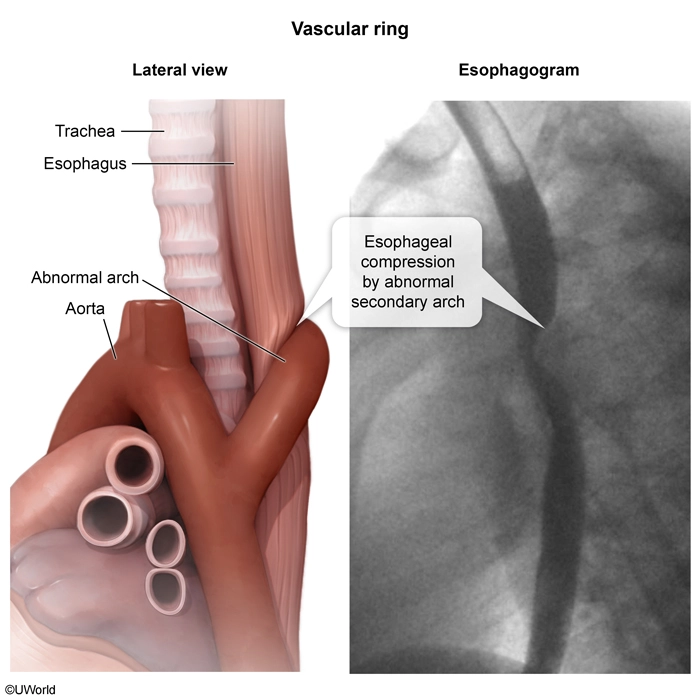
(Choice E) Vascular rings are uncommon congenital anomalies in which aortic arch vessels encircle the trachea and/or esophagus. Esophageal narrowing is expected not in the distal esophagus but rather more proximally at the level of the aortic arch.
{kind=link}
Educational objective:
Esophageal stricture is a complication of chronic gastroesophageal reflux disease and is caused by reparative collagen deposition in response to acid damage. At onset, patients have progressive dysphagia to solids but not liquids. Endoscopic findings include concentric, symmetric narrowing of the distal esophagus.
Musculoskeletal System
The musculoskeletal system makes up 8% of PANCE and PANRE. Test your exam readiness with the free musculoskeletal system sample question below.
A 30-year-old woman comes in due to pain over the lateral side of the right wrist for the last 4 days. She is 6 weeks postpartum, and the pain is worst when she lifts the infant from the crib. The patient has not had acute trauma to the wrist or hand. Examination shows tenderness over the radial side of the wrist and first dorsal compartment. With the hand in a fist and the fingers closed over the thumb, passive adduction of the wrist reproduces the pain. Which of the following is the most likely diagnosis?
| A. De Quervain tendinopathy | ||
| B. Flexor carpi radialis tenosynovitis | ||
| C. Osteoarthritis of first metacarpophalangeal joint | ||
| D. Scaphoid fracture | ||
| E. Trigger thumb |
Explanation:
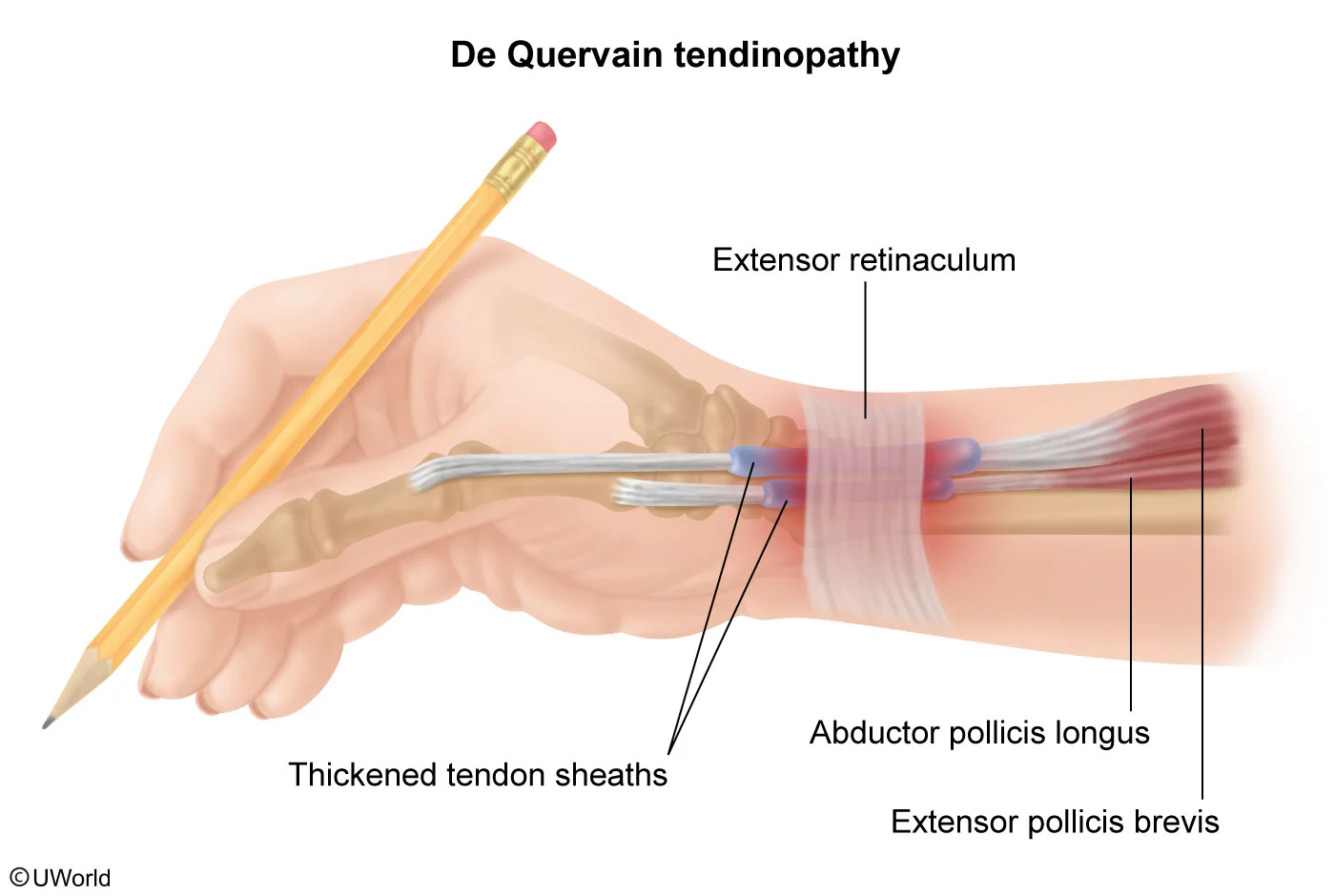
This patient has radial wrist pain consistent with de Quervain tendinopathy (DQT). DQT is an overuse syndrome involving the tendons of the abductor pollicis longus and extensor pollicis brevis and occurs most prominently at the point where the tendons pass under the extensor retinaculum in the first dorsal compartment. It most commonly occurs in women age 30-50 and is seen in higher frequencies 4-6 weeks postpartum, possibly because of repetitive thumb abduction and extension when lifting the infant.
DQT is diagnosed clinically. Examination typically shows tenderness at the radial side of the wrist at the base of the hand. In addition, reproduction of pain with the Finkelstein test (adduction of the wrist with the fingers closed over the thumb in a fist) suggests DQT. Conservative management with nonsteroidal anti-inflammatory drugs (eg, ibuprofen) and thumb spica splinting is usually adequate.
(Choice B) Flexor carpi radialis tenosynovitis is associated with excessive wrist flexion and characterized by pain and tenderness at the palmar aspect of the wrist. It is relatively uncommon; overuse of this muscle more commonly causes symptoms at the proximal origin (ie, medial epicondylitis).
(Choice C) Osteoarthritis of the first metacarpophalangeal joint causes pain over that joint, not at the carpometacarpal joint. It would be uncommon in this young patient without a history of significant trauma.
(Choice D) Scaphoid fractures typically occur during forceful hyperextension of the wrist (eg, fall on an outstretched hand). Pain and tenderness typically localize to the anatomic snuffbox.
{kind=link}
(Choice E) Stenosing tenosynovitis ("trigger thumb") results in pain over the palmar aspect of the first metacarpophalangeal joint; the pain is associated with a catching sensation during movement or locking of the thumb in flexion.
Educational objective:
De Quervain tendinopathy presents with radial wrist pain over the tendons of the abductor pollicis longus and extensor pollicis brevis. It is most common in women age 30-50, with an increased frequency during the postpartum period. Examination shows tenderness at the radial side of the wrist and a positive Finkelstein test (reproduction of pain on adduction of the wrist with the fingers closed over the thumb). Treatment includes thumb spica splinting.
Endocrine System
The endocrine system is 7% of PANCE and 8% of PANRE. See if you can answer this free endocrine system sample question.
A 27-year-old woman is seen for a pre-employment physical examination. The patient has no medical conditions but is concerned about weight gain, irregular menses, and abdominal bloating. She exercises for an hour on most days but mentions that her energy has been low. Blood pressure is 100/70 mm Hg, pulse is 86/min, and respirations are 10/min. BMI is 24.6 kg/m2. Physical examination shows dry skin, enlarged parotid glands, and knuckle abrasions on her right hand. Which of the following laboratory abnormalities is most likely to be seen in this patient?
| A. Decreased TSH level | ||
| B. Hyperchloremia | ||
| C. Hypercortisolemia | ||
| D. Hypokalemia | ||
| E. Metabolic acidosis |
Explanation:
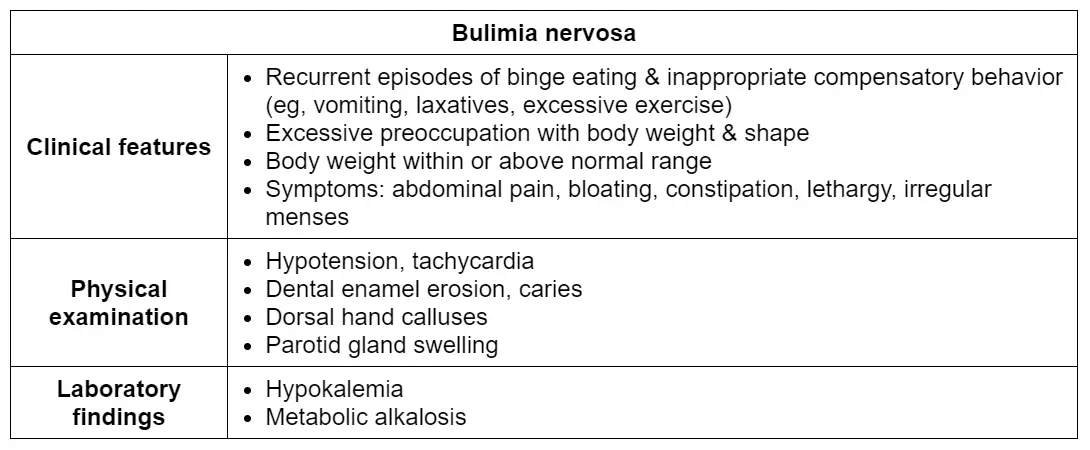
This patient's parotid gland enlargement and hand abrasions on examination are consistent with self-induced vomiting and suggest a diagnosis of bulimia nervosa (BN). This patient's concerns about weight gain and report of low energy, irregular menses, and bloating are also characteristic of this disorder. Because patients with eating disorders often attempt to hide their condition, physical examination and laboratory assessment are often key to making the diagnosis.
{kind=link}
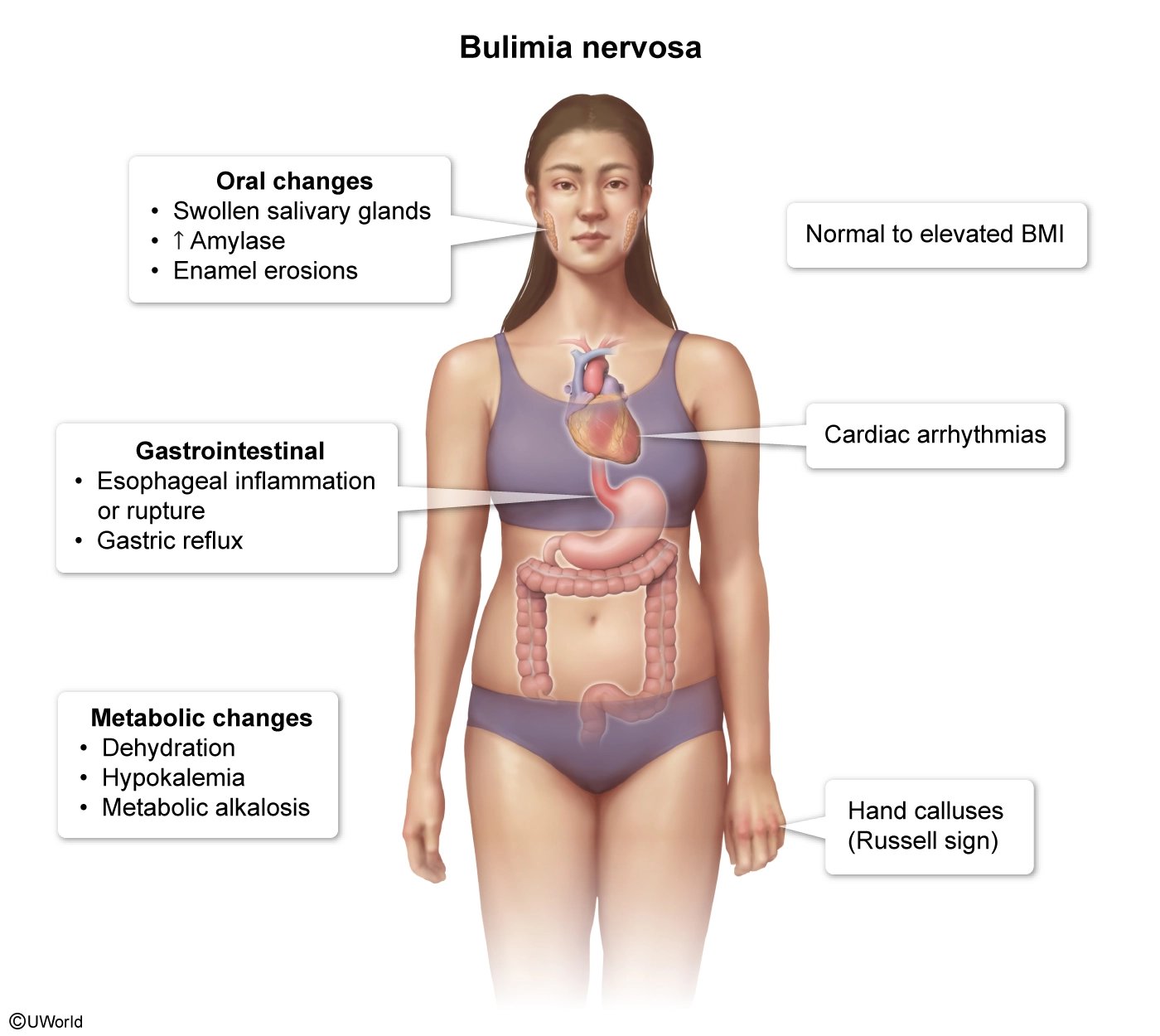
Common signs of BN include tachycardia, hypotension, dry skin, painless bilateral parotid gland swelling (possibly a response to several episodes of self-induced vomiting), calluses or scarring on the dorsum of the hand (Russell sign), and erosion of dental enamel. Electrolyte abnormalities often develop due to vomiting and include metabolic alkalosis with hypokalemia (due to renal losses of potassium in setting of alkalosis) and hypochloremia. Hypokalemia in an otherwise healthy young adult is concerning for covert BN.
(Choice A) Hyperthyroidism (evidenced by a decreased TSH level) can cause irregular menses; however, in contrast to this one, patients with hyperthyroidism also typically have weight loss and warm skin associated with increased sweating. In addition, most women with BN have normal thyroid function.
(Choices B and E) Self-induced vomiting in BN causes hypochloremia, hypokalemia, and metabolic alkalosis.
(Choice C) Although Cushing syndrome can present with weight gain, menstrual changes, decreased energy, and abdominal pain, parotid hypertrophy is more suggestive of the self-induced vomiting seen in BN.
Educational objective:
Common signs of bulimia nervosa include tachycardia, hypotension, dry skin, painless bilateral parotid gland swelling, calluses or scarring on the dorsum of the hand, and erosion of dental enamel. Laboratory abnormalities include hypokalemia, hypochloremia, and metabolic alkalosis.
Eyes, Ears, Nose, and Throat
The eyes, ears, nose and throat system makes up 7% of PANCE and 8% of PANRE. Check your eye disorders knowledge with this exam-like practice question.
A 53-year-old man comes to the clinic due to an increased difficulty reading fine print over the last year. He now must hold books, menus, and magazines at arm's length to read them. He has never had visual problems before. Which of the following is most likely abnormal in this patient?
| A. Corneal shape | ||
| B. Intraocular pressure | ||
| C. Lens elasticity | ||
| D. Lens opacity | ||
| E. Macula |
Explanation:
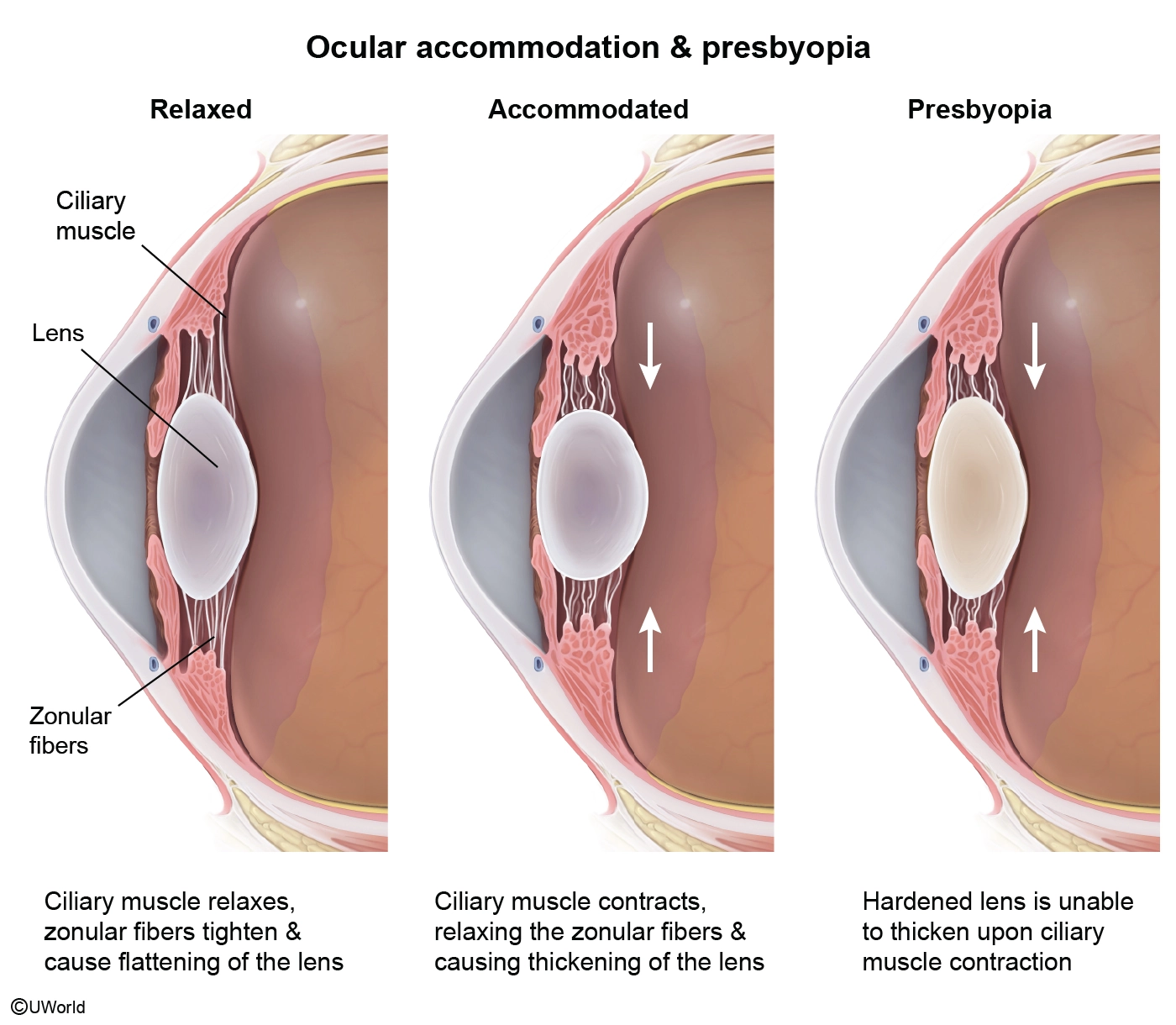
This patient is most likely suffering from presbyopia, a common age-related disorder that results from a loss of elasticity in the lens. This decrease in elasticity interferes with accommodation of the lens, which is required to focus on near objects. The tendency of patients to hold reading material at a farther distance is characteristic of presbyopia. Patients also often have no history of eye problems. Most patients report the onset of presbyopia during their 40s, and their symptoms typically peak at some point during their 60s. The poor near vision associated with presbyopia can be easily improved with reading glasses.
(Choice A) A nonspherical cornea can lead to astigmatism, which typically presents with blurry vision both at a distance and close up.
(Choice B) Elevated intraocular pressure leads to of glaucoma. Primary open-angle glaucoma usually presents with peripheral visual field defects followed by central visual field loss.
(Choice D) Increased lens opacity leads to cataracts. Patients may have difficulty reading, but a history of difficulty with night vision or driving at night is more characteristic of cataracts.
(Choice E) Age-related macular degeneration is a common cause of visual loss in patients over age 50, but it is typically associated with central visual field loss.
Educational objective:
Presbyopia is a common age-related loss of near vision caused by a decrease in lens elasticity. The classic case is a middle-aged individual who must hold books at arm's length to read.
Neurologic System
The neurologic system is 7% of PANCE and 5% of PANRE. Test your exam readiness with the free neurologic system sample question below.
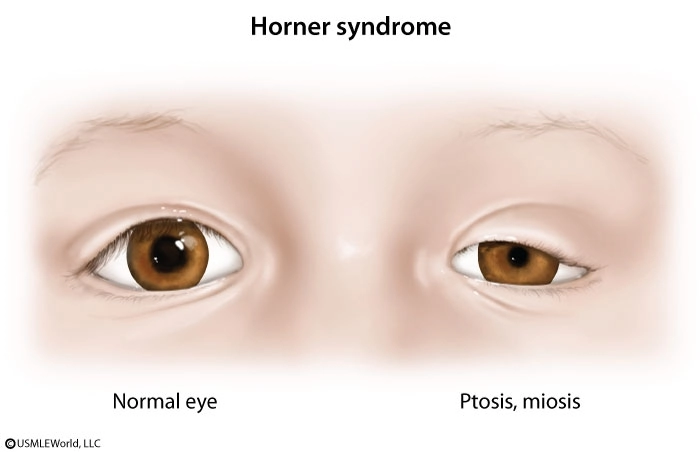
A 35-year-old man comes in for severe pain behind his left eye. The patient has had an intense, stabbing pain that woke him up around midnight. It improved after 30 minutes and he was about to go back to sleep when the same pain began again. He took ibuprofen without relief. Several months ago, the patient had similar episodes of pain that resolved spontaneously after 2 weeks. He has had no fevers, blurry vision, nausea, or vomiting but has had nasal congestion. He is a flight operations officer and says his job is stressful. Vital signs are normal. The patient is restless and agitated. Physical examination shows left-sided ptosis, miosis, and rhinorrhea. Neurologic examination shows bilateral equal and normal motor strength, sensation, and deep tendon reflexes. Which of the following is the most likely cause of this patient's headache?
| A. Brain tumor | ||
| B. Cluster headache | ||
| C. Migraine without aura | ||
| D. Tension-type headache | ||
| E. Trigeminal neuralgia |
Explanation:
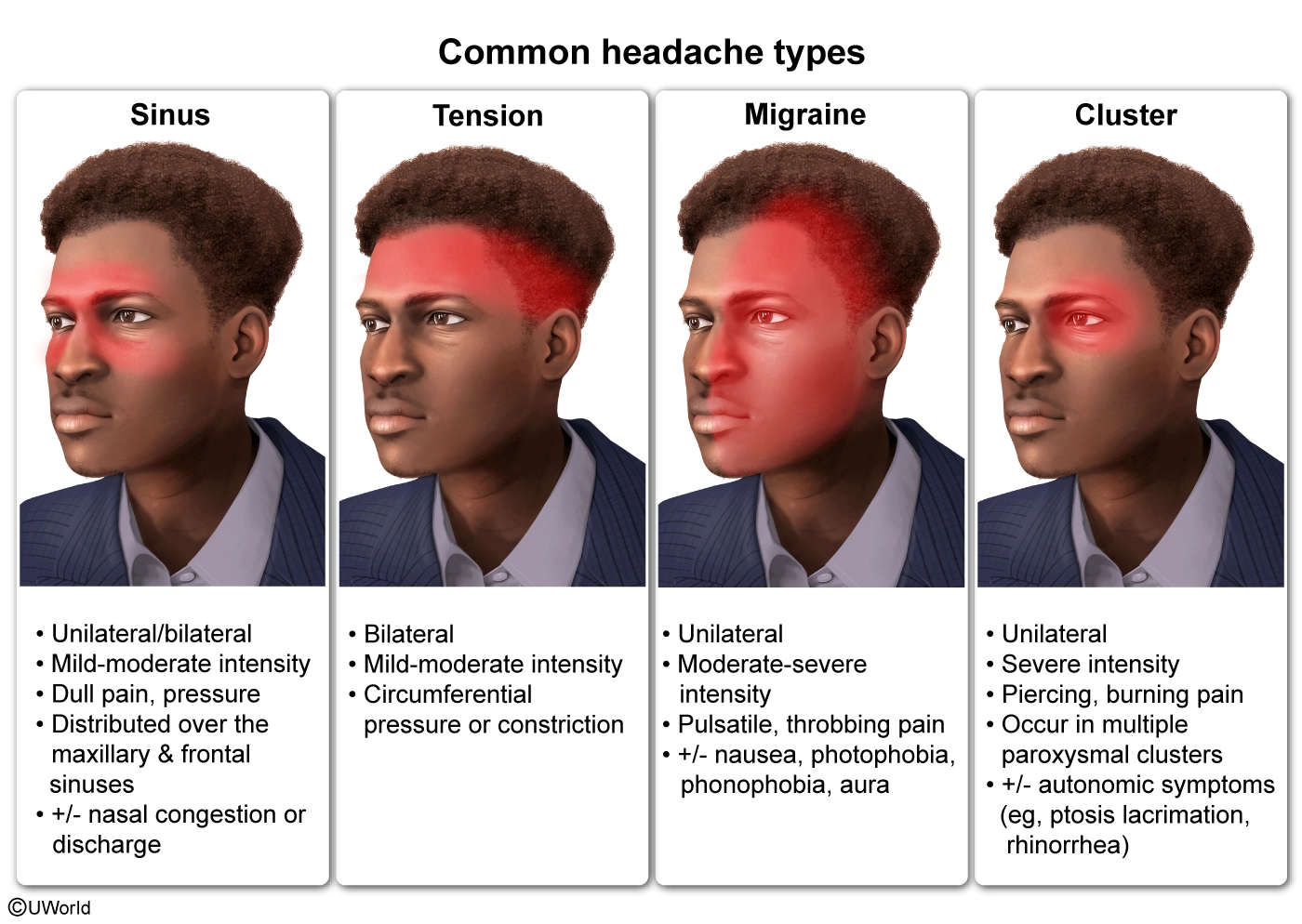
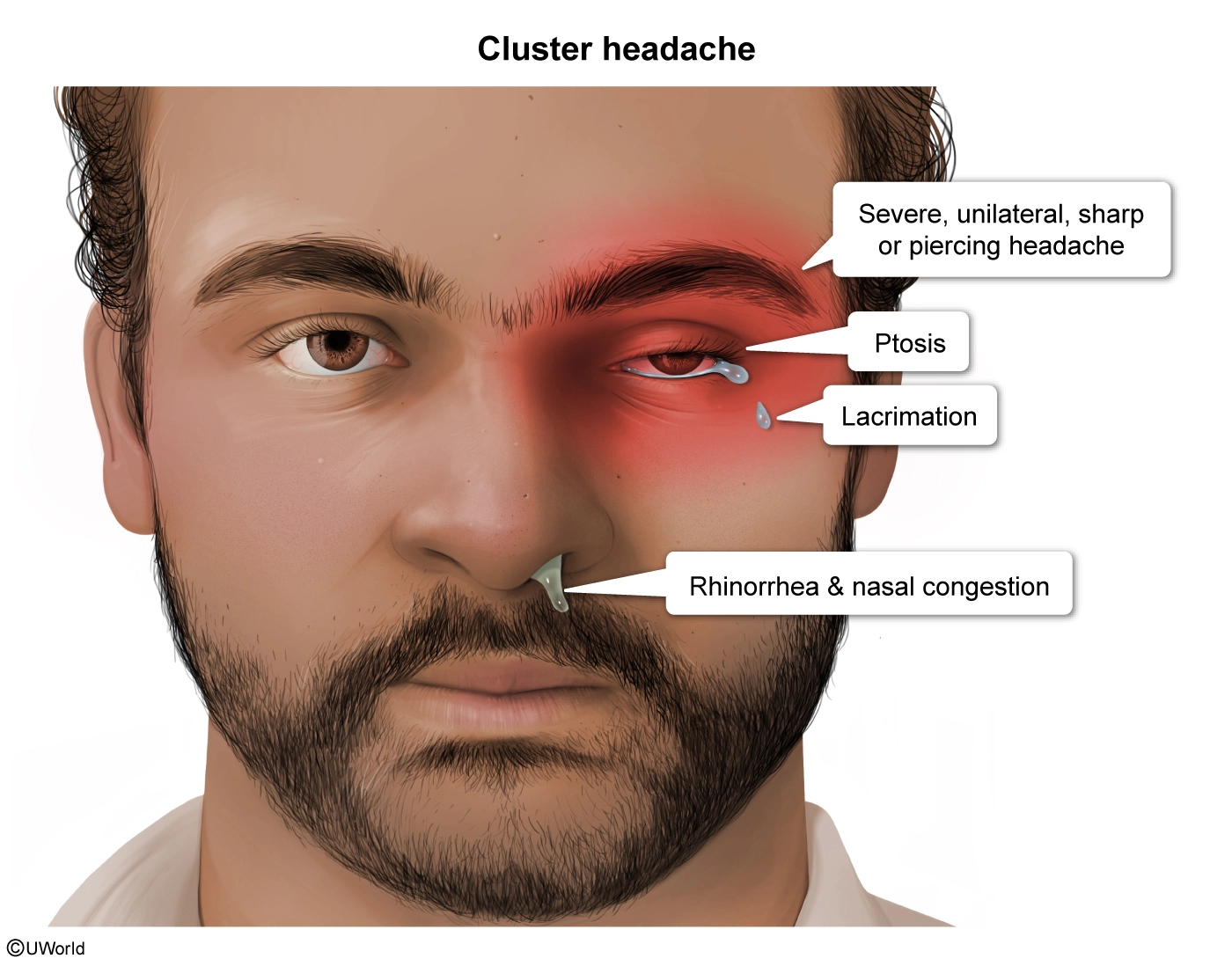
This patient with episodes of acute retro-orbital pain accompanied by ipsilateral autonomic manifestations (eg, ptosis, miosis, rhinorrhea) likely has cluster headaches. These headaches are generally seen in young men, are unilateral, and can be accompanied by redness of the ipsilateral eye with tearing but no visual changes, as well as by agitation due to the severity of the pain. The autonomic manifestations may be similar to those seen with Horner syndrome (ptosis, miosis, anhidrosis).
{kind=link}
{kind=link}
The paroxysms of cluster headache attacks begin during sleep, peak rapidly, last approximately 90 minutes, and occur up to 8 times daily for 6-8 weeks followed by a remission lasting up to a year. Because the attacks are short but severe, prophylactic medication (eg, verapamil, lithium) is important for management. An acute attack can be aborted with inhalation of 100% oxygen.
(Choices A) A brain tumor typically presents with progressive headache, morning nausea, and focal neurologic deficits due to mass effect. It does not typically cause recurrent severe retro-orbital pain in young patients.
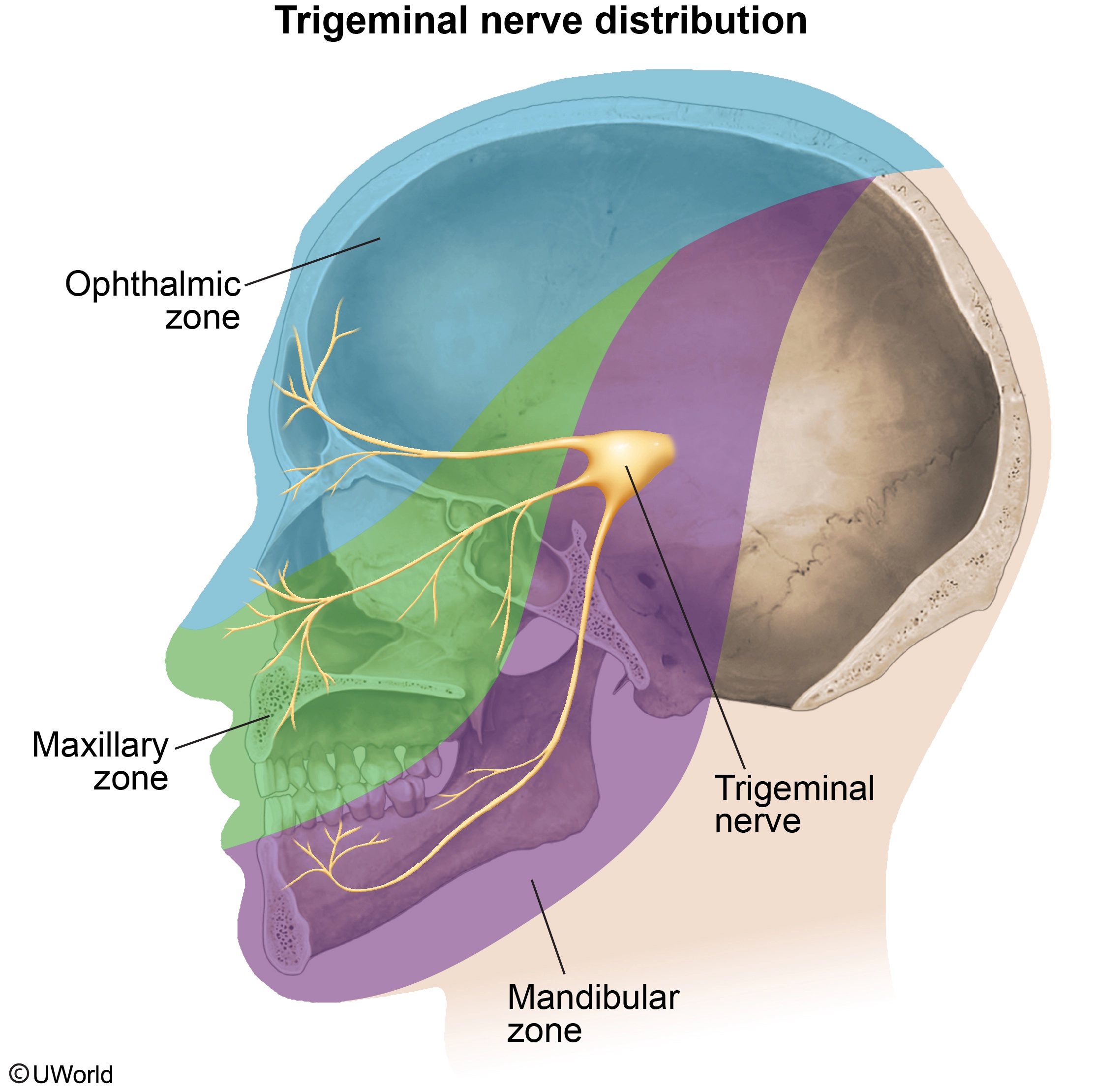
(Choices C, D, and E) Migraines are usually associated with nausea, vomiting, and photophobia; these headaches are typically pulsatile and throbbing rather than sharp and severe. Tension-type headaches can occur due to stress but are usually non-throbbing and bilateral. Trigeminal neuralgia is characterized by recurrent and sudden-onset stabbing pain along the V2 (maxillary) and V3 (mandibular) branches of the trigeminal nerve. The episodes last a few seconds to minutes and can be triggered by minor stimuli (eg, wind). Ptosis, miosis, and rhinorrhea are more suggestive of cluster headache.
{kind=link}
Educational objective:
Cluster headaches usually present with acute, unilateral, severe retro-orbital pain that awakens patients from sleep. These headaches may be accompanied by redness and tearing, rhinorrhea, and ipsilateral ptosis and miosis.

I love how the QBank sample questions challenge me and tell me why each question is wrong vs correct or which is the better answer."
Much better than other QBanks. I actually feel like I’m learning with these questions & starting with these questions is helping me do better."
Very in depth questions with different levels of difficulty. Explanations are thorough and extremely helpful."